Virtual reality won’t magically cure stigma – and sometimes it makes things worse
Primary page content
For years,virtual reality has been sold as an “empathy machine”. Put on a headset, step into someone else’s shoes, and come out a better person. Professor Sylvia Xueni Pan has spent much of her career testing that promise. Her latest work on schizophrenia suggests the hype badly needs qualifying.

The interior of a place of safety unit recreated using VR
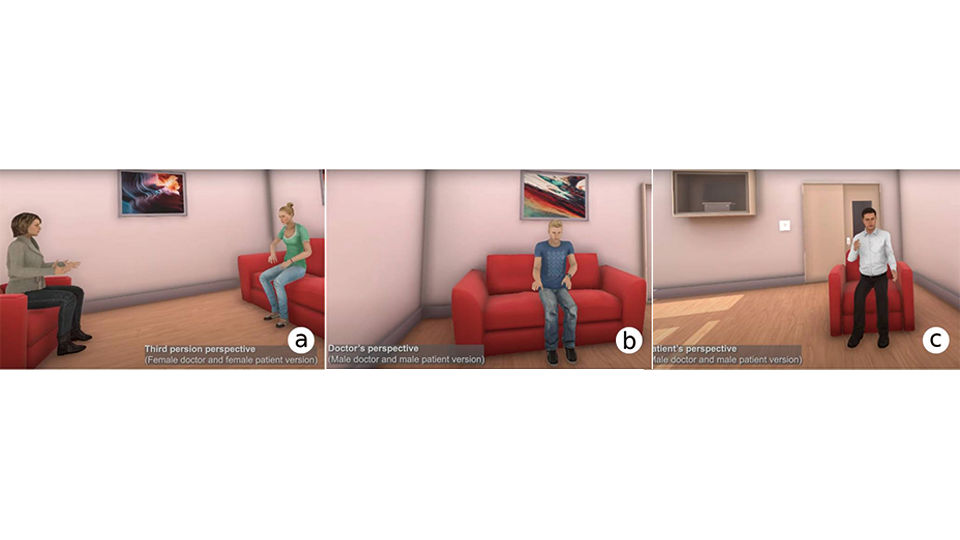
Pan and her collaborators - Jiaqi Yin and Shao-Wen Lee - built a detailed virtual re-creation of a “place of safety” unit in a Midlands hospital, where police bring people in acute psychosis for assessment. Using motion captured performances by trained actors they staged a ten minute consultation between a psychiatrist and an adolescent patient with schizophrenia.
Volunteers, mostly psychology students, experienced this consultation in VR. Crucially, they were randomly assigned to one of three viewpoints: looking on as a third person observer, embodying the doctor, or embodying the patient. Before and after the session, they completed a battery of questionnaires measuring empathy, explicit stigma and behavioural intentions such as willingness to accept someone with schizophrenia as a neighbour or marriage partner.
The headline result seems, at first glance, reassuring. “We did find that people reported more empathy afterwards,” Pan says – consistent with a large body of VR research. But looked at more closely and the picture darkens.
On several scales, including perceived recovery and social restrictions, stigma increased after the VR consultation. Participants were more inclined to see schizophrenia as hopeless and in need of tighter control, even as they claimed to understand patients better.
This, for Pan, confirms a longstanding unease about “empathy VR”. Self reported empathy, she argues, is a soft target: after any vivid experience, people will tell you they can imagine the other person’s perspective.
That doesn’t mean they are less afraid, or more willing to share their lives with them.
Sylvia Pan, Professor of Virtual Reality
The most striking finding came from the behaviour intention measures – the questions that matter most to people’s everyday lives. Here, there was a strong interaction effect depending on which body participants inhabited in VR.
Those who simply watched from the sidelines came out with higher stigma: greater social distance, more restrictive attitudes. Those who embodied the patient showed little overall change. But those who became the doctor showed a reduction in stigma on some key behavioural items.
“In a way, the first two results are about VR in general,” Pan explains. “You get more empathy, but also more bias. The embodiment result is the interesting one: putting people in the shoes of the effective professional in a successful consultation seems to nudge them towards less stigma.”
An implicit attitude test (IAT) tailored to mental health failed to show a clear shift, but Pan is cautious about interpreting that null result. Unlike race, schizophrenia is hard to represent visually, and the task design may not yet be sensitive enough to detect subtle changes.
What her study does show, she insists, is that VR is a double-edged sword. If you faithfully portray a distressing, disorganised psychotic episode, “you may increase people’s sense of how frightening and unpredictable it is,” Pan observed, and thereby worsen stigma – particularly among groups, such as nurses, who already face the brunt of violent or chaotic behaviour on wards.
A related project with longtime collaborator Professor Mel Slater at the University of Barcelona underlines the point. There, participants “time travelled” through their own life in VR under climate change: as a child in a greener past, a young adult in an anxious present, a parent in a damaged near future, and an older adult in a brighter world achieved through collective action. Those who embodied themselves at each stage showed a short term reduction in carbon footprint two weeks later; those who merely observed did not. By six weeks, however, the effect had faded.
Across both studies, a common lesson emerges: VR doesn’t automatically make people more virtuous. It amplifies whatever script you build – the role you assign the user, the tone of the encounter, whether the story ends in paralysis or agency.
Pan’s message to policymakers and practitioners is not to abandon VR, but to use it with care and in collaboration. “It’s a powerful tool,” she says. “But you can’t just throw VR at stigma or climate change and assume it will help. You have to design the experience around competence, agency and realistic hope – and you have to keep testing that it’s doing what you think it’s doing.”